


Results of screening for antibodies to varicella-zoster virus in healthcare workers of a multidisciplinary hospital in Moscow
- Authors: Afonina N.M.1, Mikheeva I.V.1, Korabelnikova M.I.1, Rodionova Z.S.1, Snitsar A.V.2,3, Perekhodov S.N.3, Smetanina S.V.2, Tutelyan A.V.1, Kuzin S.N.1, Akimkin V.G.1
-
Affiliations:
- Central Research Institute of Epidemiology
- City Clinical Hospital named after V.P. Demikhov
- A.I. Yevdokimov Moscow State University of Medicine and Dentistry
- Issue: Vol 100, No 6 (2023)
- Pages: 410-419
- Section: ORIGINAL RESEARCHES
- URL: https://microbiol.crie.ru/jour/article/view/18513
- DOI: https://doi.org/10.36233/0372-9311-427
- EDN: https://elibrary.ru/vfdotz
- ID: 18513

Cite item

Abstract
Introduction. Given the unfavorable epidemic situation with chickenpox and shingles in Russia, there is a high risk of virus introduction and spread in healthcare settings, including among medical staff who are not immune to varicella zoster virus (VZV).
The objective of this study is to assess the immunity of employees of a multidisciplinary hospital in Moscow to VZV.
Materials and methods. A selective screening study was carried out. Venous blood serum samples were taken from 1546 hospital employees as material for detection of IgG antibodies to VZV antigens using a commercial solid-phase enzyme immunoassay (ELISA) test system "Vecto VZV-IgG". All employees were questioned to obtain information about their infectious and vaccine history in relation to VZV.
Results and discussion. Screening for antibodies to VZV in the hospital workers revealed that 6.3% of those workers are not immune to VZV. The proportion of seronegative individuals was the highest (12.6 ± 2.4%) in the age group of 29 years and younger. VZV seronegative healthcare workers were found in various departments, but the presence of non-immune individuals among the staff of the obstetrics and gynecology departments (6.5%) is of epidemiologic concern. The results of the survey showed that documented data on infection and vaccination history cannot be used to assess the protection of healthcare workers against VZV infection.
Conclusion. The results of serologic screening for antibodies to VZV made it possible to identify a significant number of susceptible employees of the multidisciplinary hospital. In order to prevent the formation of multiple epidemic foci of varicella in medical organizations, it is advisable to include anti-VZV testing of medical staff in the state prevention programs with subsequent vaccination of non-immune individuals.
Full Text
Introduction
Despite significant advances in infection control at healthcare organizations (HCOs) through a wide range of sanitary and epidemiological measures and preventive vaccination, infectious diseases still pose a serious threat to patients and healthcare staff. In this regard, attention should be focused on HCO employees who have not previously contracted vaccine-preventable diseases and have not been vaccinated before entering the workplace, as they are at risk of infection and subsequently at risk of becoming a source of the pathogen for susceptible seronegative patients [1].
In Russia, the most widespread infectious diseases (apart from acute respiratory viral infections) are diseases caused by Varicella zoster virus (VZV) — chickenpox and shingles. In 2022, more than 648,000 cases of chickenpox and 16,680 cases of shingles were registered in the country. Children account for the majority of cases of chickenpox (95.6%), and adults account for 91.5% of the age structure of patients with shingles [2].
In the current epidemic situation in the HCO, there is a high risk of VZV entry and spread, including among medical staff who are non-immune to VZV.
There are no precise statistical data on the frequency of hospitalization of chickenpox and shingles patients in Russia. At the same time, when studying the frequency of hospitalization of herpesvirus patients in the Moscow Infectious Diseases Clinical Hospital No. 1 for the years 2010–2021, the predominance of hospitalized VZV-infected adults was established: 5162 adults with VZV (4705 — diagnosed with shingles and 357 — with chickenpox) [3] and 226 children (196 — diagnosed with chickenpox and 30 — with shingles) were hospitalized during the studied period [4].
Foreign literature has published data that the circulation of VZV in pediatric HCOs is decreasing due to the infrequent hospitalization of children for chickenpox due to routine preventive vaccination for chickenpox in the pediatric population [5]. However, VZV is actively circulating in adult HCOs and the source of the pathogen is predominantly patients with shingles [6-9]. Due to erroneous stereotypical beliefs that chickenpox is predominantly a pediatric disease and infection is only spread from chickenpox patients, those with shingles are often overlooked as VZV sources. For this reason, the risks of infection and spread of chickenpox in adult HCOs are underestimated.
Chickenpox in patients with hospital-acquired infections is characterized by high intensity of spread, aggravation of the course and development of complications [10]. Foreign authors have noted that outbreaks of chickenpox in hospitalized patients are associated not only with severe consequences for patients, but also with a significant financial burden for the hospital, as well as with lawsuits from exposed patients [11, 12].
In this regard, it is extremely important to exclude the possibility of spreading chickenpox among non-immune medical staff, therefore, immunization against chickenpox in a number of countries is regulated for seronegative employees [13, 14].
In Russia, despite the unfavorable epidemic situation with chickenpox and shingles, healthcare workers do not undergo mandatory serological testing for antibodies to VZV with subsequent vaccination of non-immune workers and there is no data on the immunity to the chickenpox pathogen in this group of the increased occupational risk of infection.
At the same time, the World Health Organization recommends immunization against chickenpox in non-immune healthcare workers [15].
Taking into account the relevance of the problem, a study was conducted to assess the immunity of employees of a multidisciplinary hospital in Moscow to VZV.
Materials and methods
A selective screening study was conducted. In the year 2021, venous blood serum samples were taken from 1546 hospital employees of one of the multidisciplinary hospitals in Moscow as material for this study. All employees gave voluntary informed written consent to participate in the study. The study protocol was approved by the Ethical Committee of the Central Research Institute of Epidemiology of Rospotrebnadzor (protocol No. 114 of 22.04.2021). The socio-demographic characteristics of the clinical study group are presented in Table 1.
Table 1. Characteristics of the studied group (n = 1546)
Parameter | Number of respondents | ||
abs. | % | ||
Sex | women | 1338 | 86,5 |
men | 208 | 13,5 | |
Age, years | ≤ 29 | 190 | 12,3 |
30–39 | 350 | 22,6 | |
40–49 | 413 | 26,7 | |
50–59 | 372 | 24,1 | |
> 60 | 221 | 14,3 | |
Work experience, years | < 10 | 454 | 29,3 |
10-20 | 360 | 23,4 | |
20-30 | 309 | 19,9 | |
> 30 | 304 | 19,7 | |
not indicated | 119 | 7,7 | |
The qualitative detection of IgG antibodies to VZV antigens was performed using a commercial solid-phase enzyme-linked immunosorbent assay (ELISA) test system "Vecto VZV-IgG". The testing was performed according to the screening method in a single dilution (1 : 100) of serum samples. In accordance with the instructions to the test system, the obtained results were interpreted as positive or negative when correlating the testing results to the manufacturer’s standard panel with or without IgG antibodies to VZV.
The study also included a questionnaire survey of all employees to obtain information on infection and vaccine history related to VZV.
Confidence intervals with a significance level of 95% were calculated to assess the statistical significance of differences in relative indices. Graphical processing of the data was performed using the MS Excel program.
Results
Among the staff of a multidisciplinary hospital in Moscow, 1448 (93.4%) employees immune to VZV and 98 (6.3%) employees without antibodies to VZV were identified.
The proportion of seronegative individuals among women and men was almost the same: among women – 6.7 ± 1.4% (n = 89), among men – 4.3 ± 0.7% (n = 9), the difference of indicators was statistically unreliable (t = 1.6; p ≤ 0.05).
The analysis of the VZV immunity level by age groups showed that in the group up to 29 years of age, every 8th hospital employee lacked the antibodies to VZV (24 out of 190), and in the age group over 30 years of age, it was every 18th employee (74 out of 1356).
The proportion of VZV seropositive healthcare workers in the age group of 30 years and older was 94.5 ± 0.6%, which was significantly higher than in the group of young healthcare workers up to 29 years of age (87.4 ± 2.4%; t = 2.7; p ≤ 0.05). Within the age group of 30 years and older, seropositivity rates had no statistically significant differences (Fig. 1).

Fig. 1. The proportion of VZV seropositive cases in different age groups of healthcare workers of a multidisciplinary hospital in Moscow.
The results of the study indicate a higher probability of chickenpox in young specialists compared to older medical workers.
In order to assess the risk of infection of seronegative individuals during the work period in the HCO, the immunity was assessed in groups of staff, depending on the years of service in the specialty.
In the groups of hospital staff with less than 10 and up to 20 years of service in the HCO, the proportion of individuals without antibodies to VZV was higher than among staff with 20-30 and more than 30 years of service: 6.4 ± 1.1 and 8.3 ± 1.5% vs. 3.9 ± 1.1 and 4.3 ± 1.2%, respectively (p ≤ 0.05; Fig. 2).

Fig. 2. The proportion of VZV seronegative healthcare workers of a multidisciplinary hospital in Moscow, depending on the years of service.
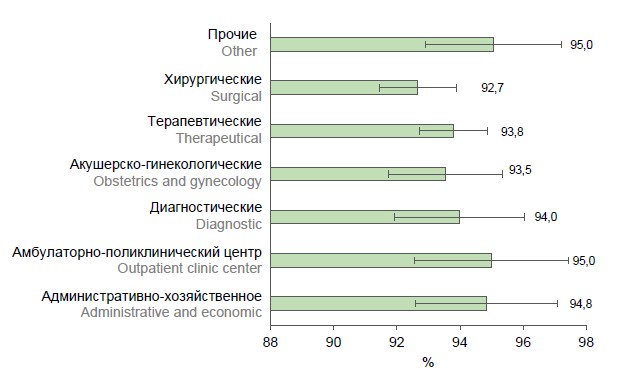
VZV seronegative healthcare workers were found in all hospital departments. The immunity to VZV in different departments ranged from 92.7% in surgical departments to 95.0% in the outpatient center and other departments. Statistical processing of the results showed that there was no significant difference between the proportion of seronegative/seropositive workers in different hospital departments (p ≤ 0.05; Table 2; Fig. 3).
Table 2. Results of serological testing for antibodies to VZV of healthcare workers in various departments of a multidisciplinary hospital in Moscow
Department profile | Number of examined persons | ||||
total | of which seronegative | of which seroposive | |||
abs. | % (Р ± mр) | abs. | % (Р ± mр) | ||
Surgical | 450 | 33 | 7,3 ± 1,2 | 417 | 92,7 ± 1,2 |
Obstetrics and gynecology | 186 | 12 | 6,5 ± 1,8 | 174 | 93,5 ± 1,8 |
Therapeutical | 499 | 31 | 6,2 ± 1,1 | 468 | 93,8 ± 1,1 |
Diagnostic | 133 | 8 | 6,0 ± 2,1 | 125 | 94,0 ± 2,1 |
Administrative and economic | 97 | 5 | 5,2 ± 2,2 | 92 | 94,8 ± 2,2 |
Outpatient clinic center | 80 | 4 | 5,0 ± 2,4 | 86 | 95,0 ± 2,4 |
Other (reception, narcological, etc.) | 101 | 5 | 5,0 ± 2,2 | 96 | 95,0 ± 2,2 |
Total | 1546 | 98 | 6,3 | 1448 | 93,4 |

Fig. 3. The proportion of VZV seropositive healthcare workers in various departments of a multidisciplinary hospital in Moscow.
In this study, the infectious history of healthcare workers and vaccination history related to chickenpox were studied. Due to the lack of documents confirming the fact of disease or vaccination (chickenpox recovery and immunization certificates), the assessment was based on a questionnaire survey of healthcare workers (1546 respondents).
About 40% of health workers (604 respondents) reported that they had previously experienced chickenpox, 42% (666 respondents) did not know about their infection and vaccination history, and 18% (276) considered themselves vaccinated against chickenpox. Employees of the therapeutic, obstetrics and gynecology departments considered themselves vaccinated in a significantly lower proportion of cases (7.0% and 4.8%, respectively) compared to employees of other departments (19.3% in surgical departments, 42.9% in diagnostic departments, 33% in administrative departments, and 41.6% in other departments); the differences were statistically significant (p < 0.05). Taking into account the absence of vaccination against chickenpox in the National Immunization Calendar of Russia, as well as insignificant volumes of vaccination against this infection by epidemic indications, the adequacy of the obtained employee questionnaire results regarding previous vaccination against chickenpox is questionable. The unreliability of the vaccination history was indirectly confirmed by the almost identical proportion of seronegative individuals among the supposedly vaccinated and those with an unknown history: 8.7 ± 1.7 and 9.9 ± 1.2%, respectively (t = 0.6; p ≤ 0.05).
Comparison of the questionnaire data with the results of serologic screening showed that 1.3 ± 0.5% of individuals without antibodies to VZV were found among healthcare workers who considered themselves to have been previously infected with chickenpox, while 6.5 times more seronegative persons were found among those who reported being vaccinated against chickenpox (8.7 ± 1.7%; t = 4.1; p ≤ 0.05; Table 3).
Table 3. Results of serological screening of medical workers with various infectious and vaccine histories regarding chickenpox based on the results of a questionnaire
Anamnesis based on the results of the questionnaire | Number of respondents | ||
total | of which seronegative | ||
abs. | % (Р ± mр) | ||
Have had chickenpox before | 604 | 8 | 1,3 ± 0,5 |
Consider themselves vaccinated against chickenpox | 276 | 24 | 8,7 ± 1,7 |
Have no information | 666 | 66 | 9,9 ± 1,2 |
Total | 1546 | 98 | 6,3 |
Discussion
Screening for antibodies to VZV in medical workers of a multidisciplinary hospital revealed a high proportion of seropositive individuals (93.7%). Taking into account that the study involved individuals of a certain vulnerable population group (employees of the HCO), we did not extrapolate the results of the screening to the adult population of the country. At the same time, the obtained result is comparable with the data of population studies on assessment of immunity to VZV in European countries, indicating that more than 90% of adults in most of them are VZV seropositive. At the same time, the level of adult seropositivity is higher than in most Asian countries with warmer climates (India — 68.2%, Turkey — 77.8%, Thailand — 61.4%, Iran — 78.5%, etc.) [16].
Despite the high level of herd immunity to VZV identified in this study, the probability of infection of healthcare workers in the event of the pathogen introduction was shown: 98 medical staff did not have immunity to VZV. At the same time, in the case of chickenpox infection, medical staff may become a source of the infection for weakened in-patients, whose chickenpox is extremely severe.
The probability of VZV infection spread and the formation of multiple foci of VZV infection among the staff and patients of multidisciplinary hospitals is proved by the results of an assessment of the nosocomial incidence of chickenpox infection in the Moscow HCO [17, 18].
The risk of VZV entry into non-infectious adult hospitals is evidenced by the data on the frequency of hospitalization of patients with shingles, which are the sources of the chickenpox pathogen. In particular, our earlier epidemiological study showed that in Moscow, 30% of all patients with shingles (more than 300 people annually) were admitted to hospitals, and in the vast majority of cases, admitted to non-infectious wards [17].
The results obtained, which demonstrated that there was no statistically significant difference in the proportion of seronegative/seropositive individuals among women and men in the studied cohort, are consistent with the literature data that chickenpox occurs with equal frequency in males and females [19], as well as with the results of serologic studies indicating that there is no difference in the proportion of VZV seropositive cases among individuals of different sexes [16].
The study of the immunity by age groups, which showed that the proportion of VZV seropositive individuals in the age group up to 29 years of age was significantly lower than among medical staff 30 years and older (87.4 ± 2.7 vs. 94.5 ± 0.6%), confirmed the previously published serosurvey data on the increase in the proportion of VZV seropositive individuals with age [16, 20]. Comparable results were also obtained in 2014 when studying the immunity of the Moscow population to VZV: among adults of childbearing age aged 20-29 years, the proportion of seropositive individuals was 88.2 ± 5.5% [21].
The data obtained objectively indicate the presence of a higher probability of chickenpox disease in young hospital staff compared to healthcare workers from older age groups. However, taking into account the age structure of the hospital staff, in which the proportion of persons aged 30 years and older was more than 87% (Table 1), the number of persons without detectable antibodies to VZV among mature-age persons was significant in absolute terms: 74 out of 98 non-immune persons detected. Therefore, when conducting anti-epidemic measures in case of chickenpox introduction into the hospital from the groups at risk of disease development, medical workers of older age groups cannot be excluded.
Working in a non-infectious HCO is itself a factor of increased risk of contact with a patient with inapparent or latent VZV infection. However, data from this study has shown that many years of service in the HCO is not a definite evidence of post-infection immunity to chickenpox infection, because among the employees with more than 20 years of service there were found persons without antibodies to the chickenpox pathogen.
When studying the immunity of healthcare workers of different departments of a multidisciplinary hospital, approximately the same proportion of employees immune to VZV was established. At the same time, it is known that the probability of VZV introduction is higher in those departments of a multidisciplinary hospital where patients with clinical manifestations characteristic of shingles are hospitalized. The most frequent complications of shingles requiring hospitalization of patients are post-herpetic neuralgia, bacterial infections, eye damage, neurological complications and generalization of infection. Moreover, among elderly individuals with shingles, the incidence of hospitalization is increasing annually [20]. Thus, the risks of VZV infection are higher in wards with a high proportion of elderly patients (therapeutic and neurological wards), as well as in wards and hospitals with long stays of debilitated patients (psychiatric and phthisiatric wards).
The presence of non-immune staff in obstetrics and gynecology departments (12 people; 6.5%), where the risk of chickenpox outbreaks is associated with the risk of infection of pregnant women and newborns, should be of particular epidemiologic concern.
In a study conducted in Poland, which included questionnaires and serologic screening for IgG antibodies to VZV of 524 physicians, midwives, and nurses in maternity, neonatal and pediatric units, 14.7% of potentially seronegative healthcare workers were identified, which was twice as high as in our study [22]. We assume that this is due to different methods of assessing the state of humoral immunity: in our study, only qualitative assessment (positive or negative for IgG antibodies to VZV) was performed and the level of immunity was not taken into account. However, in the study described above, quantitative assessment was performed and employees with a concentration of specific IgG antibodies ≥ 5 IU/mL were classified as seropositive individuals [22]. Thus, the influence on the results of serologic screening of the selected methodology of antibody detection and sensitivity of the employed ELISA test systems should be taken into account.
Comparison of the questionnaire data of medical staff conducted within the framework of the present study with the results of serologic screening shows the unreliability of the anamnestic data not supported by documents. This is demonstrated both by the almost equal percentage of seronegative persons among those supposedly vaccinated and those with unknown history, and by the detection of seronegative persons in the group of those who had been previously infected.
We believe that the information on previous vaccination against chickenpox obtained during the employee questionnaire does not reflect the true situation, since the National Immunization Calendar of Russia does not provide for routine vaccination against chickenpox, and vaccinations against this infection have been carried out since 2013 to a very limited contingent of risk groups, not including healthcare workers. It is likely that some employees may mistakenly believe that they have been immunized against chickenpox without documentation of their preventive vaccinations. However, this may indirectly indicate a lack of competence of healthcare professionals in the field of immunoprophylaxis of infectious diseases.
Previous studies have shown that, due to the possibility of an inapparent course of chickenpox, the absence of a history of chickenpox is not necessarily associated with the absence of IgG antibodies to VZV [21], and the presence of this infection in the history does not guarantee the presence of antibodies due to possible clinical diagnostic errors in the absence of laboratory confirmation of the diagnosis [21, 22].
Thus, in the course of the questionnaire survey it was demonstrated that medical workers are not always able to present their reliable infection and vaccination history, and its objective confirmation can be obtained only by testing for antibodies to VZV.
In the absence of routine vaccine prophylaxis to prevent nosocomial spread of infection, it seems reasonable to organize serological monitoring of immunity to VZV through a single test (screening) of all employees, and in the future, on a regular basis, to conduct serological examination only of persons newly hired to work in the HCO. Detected seronegative persons should be vaccinated against chickenpox regardless of age. Such an approach will significantly reduce the costs of anti-epidemic measures in case of VZV introduction into the HCO, as well as reduce the risk of pathogen entry due to the disease of employees.
Immunization against chickenpox, recommended by WHO since the 1990s, is the gold standard for chickenpox prophylaxis. Currently, WHO recommends immunization against chickenpox for all healthcare workers who are not immune to VZV, but if it is not economically feasible, only staff in obstetrics and gynecology departments may be immunized, because chickenpox poses a serious threat to maternal, fetal and neonatal health and because of the fact that post-exposure immunization of pregnant women is not possible [15].
In the European region, 13 countries recommend immunization against chickenpox for healthcare workers who have not been serologically tested for antibodies to VZV[1].
In the United States, all healthcare staff should have documented immunity to VZV, as evidenced by either double immunization against chickenpox, the presence of antibodies to VZV, or a physician-confirmed history of chickenpox or shingles [14].
Domestic authors have also indicated that it is advisable to vaccinate healthcare workers who have not previously had chickenpox [10]. However, the issues of laboratory confirmation of immunity to VZV are still unresolved in Russian healthcare practice.
Given the difficulties in procuring foreign vaccines for chickenpox prophylaxis and test systems to determine the level of immunity to VZV, the development and introduction of domestic test systems and domestic chickenpox vaccines into the public health practice is crucial for the implementation of such an initiative.
Summary of results
- Serologic screening for antibodies to VZV showed both a high level of herd immunity (93.7%) among medical staff of a multidisciplinary hospital in Moscow and the presence of seronegative individuals susceptible to chickenpox among employees of various departments, all age groups and with different years of service.
- Significantly more VZV seronegative individuals were found among staff under 29 years of age than among healthcare workers in older age groups and with more years of service.
- The level of immunity to VZV was found to be approximately the same among multidisciplinary hospital workers of different departments.
- The questionnaire demonstrated that healthcare workers could not present their reliable infection and vaccination history regarding chickenpox, and its objective confirmation could only be obtained by testing for antibodies to VZV.
- The necessity of introducing preventive vaccination against chickenpox, including in medical workers, as well as the relevance of creating a serological monitoring system of immunity to VZV in employees of the HCO in order to prevent the entry of the pathogen and to optimize anti-epidemic measures in case of infection outbreak are shown.
Conclusion
The results of serologic screening for antibodies to VZV revealed the presence of susceptible individuals among the staff of a multidisciplinary hospital, which indicates the presence of conditions for the pathogen introduction with sick medical staff and the formation of epidemic foci of chickenpox in non-infectious HCOs.
Taking into account the obtained results, it is necessary to develop and put into practice domestic vaccines against chickenpox, as well as domestic test systems for serosurveillance of VZV infection. At the initial stage of introducing preventive vaccination for chickenpox, it is advisable to conduct serologic testing for antibodies to VZV in medical staff with subsequent vaccination of non-immune individuals.
In the context of planning the inclusion of vaccinations against chickenpox in the National Immunization Calendar of Russia, the obtained data are of interest regarding the use of serologic methods to assess the prevalence of VZV infection in order to obtain data on the disease risk groups and improve measures to counteract the infection.
1 European Centre for Disease Prevention and Control, Varicella vaccination in the European Union. Stockholm ECDC. 2015. URL: https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Publications/Varicella-Guidance-2015.pdf (дата обращения: 13.05.2023).
About the authors
Nataliya M. Afonina
Central Research Institute of Epidemiology
Email: irina_mikheeva@mail.ru
ORCID iD: 0000-0002-3205-4025
Cand. Sci. (Med.), researcher, Laboratory of immunization
Russian Federation, MoscowIrina V. Mikheeva
Central Research Institute of Epidemiology
Author for correspondence.
Email: irina_mikheeva@mail.ru
ORCID iD: 0000-0001-8736-4007
D. Sci. (Med.), Professor, Head, Laboratory of immunoprophylaxis
Russian Federation, MoscowMarina I. Korabelnikova
Central Research Institute of Epidemiology
Email: irina_mikheeva@mail.ru
ORCID iD: 0000-0002-2575-8569
researcher, Laboratory of viral hepatitis
Russian Federation, MoscowZinaida S. Rodionova
Central Research Institute of Epidemiology
Email: irina_mikheeva@mail.ru
ORCID iD: 0000-0003-0401-279X
researcher, Laboratory of viral hepatitis
Russian Federation, MoscowArtem V. Snitsar
City Clinical Hospital named after V.P. Demikhov; A.I. Yevdokimov Moscow State University of Medicine and Dentistry
Email: irina_mikheeva@mail.ru
ORCID iD: 0000-0001-6053-4651
deputy chief physician
Russian Federation, Moscow; MoscowSergey N. Perekhodov
A.I. Yevdokimov Moscow State University of Medicine and Dentistry
Email: irina_mikheeva@mail.ru
ORCID iD: 0000-0002-6192-2581
D. Sci. (Med.), Professor, Head, Department of hospital surgery
Russian Federation, MoscowSvetlana V. Smetanina
City Clinical Hospital named after V.P. Demikhov
Email: irina_mikheeva@mail.ru
ORCID iD: 0000-0003-3763-697X
Cand. Sci. (Med.), Сhief doctor
Russian Federation, MoscowAlexey V. Tutelyan
Central Research Institute of Epidemiology
Email: irina_mikheeva@mail.ru
ORCID iD: 0000-0002-2706-6689
D. Sci. (Med.), Professor, Corresponding Member of the Russian Academy of Sciences, Head, Laboratory for healthcare-related infections
Russian Federation, MoscowStanislav N. Kuzin
Central Research Institute of Epidemiology
Email: irina_mikheeva@mail.ru
ORCID iD: 0000-0002-0616-9777
D. Sci. (Med.), Professor, Head, Viral hepatitis laboratory
Russian Federation, MoscowVasily G. Akimkin
Central Research Institute of Epidemiology
Email: irina_mikheeva@mail.ru
ORCID iD: 0000-0001-8139-0247
D. Sci. (Med.), Professor, Academician of the Russian Academy of Sciences, Director
Russian Federation, MoscowReferences
- Sydnor E., Perl T.M. Healthcare providers as sources of vaccine-preventable diseases. Vaccine. 2014;32(38):4814–22. DOI: https://doi.org/10.1016/j.vaccine.2014.03.097
- Государственный доклад «О состоянии санитарно-эпидемиологического благополучия в Российской Федерации в 2022 году». М.; 2023.
- Орадовская И.В., Викулов Г.Х., Колобухина Л.В. и др. Герпесвирусные инфекции у взрослых жителей г. Москвы: заболеваемость, распространенность, нозологические формы и алгоритм ведения. Инфекционные болезни. 2022;20(4): 125–42. Oradovskaya I.V., Vikulov G.Kh., Kolobukhina L.V., et al. Herpesvirus infections in adult residents of Moscow: incidence, prevalence, nosological forms and algorithm of management. Infectious Diseases. 2022;20(4):125–42. DOI: https://doi.org/10.20953/1729-9225-2022-4-125-142
- Викулов Г.Х., Орадовская И.В., Колобухина Л.В. Герпесвирусные инфекции у детей: распространенность, заболеваемость, клинические формы и алгоритмы ведения. Вопросы практической педиатрии. 2022;17(6):125–142. Vikulov G.Kh., Oradovskaya I.V., Kolobukhina L.V. Herpesvirus infections in children: prevalence, incidence, clinical forms, and management algorithm. Clinical Practice in Pediatrics. 2022;17(6):125–142. DOI: https://doi.org/10.20953/1817-7646-2022-6-126-140
- Helmuth I.G., Poulsen A., Suppli C.H., Mølbak K. Affiliations expand Varicella in Europe-A review of the epidemiology and experience with vaccination. Vaccine. 2015;33(21):2406–13. DOI: https://doi.org/10.1016/j.vaccine.2015.03.055
- Breuer J. Herpes zoster: new insights provide an important wake-up call for management of nosocomial transmission. J. Infect. Dis. 2008;197(5):635–7. DOI: https://doi.org/10.1086/527421
- Johnson J.A., Bloch K.C., Dang B.N. Varicella reinfection in a seropositive physician following occupational exposure to localized zoster. Clin. Infect. Dis. 2011;52(7):907–9. DOI: https://doi.org/10.1093/cid/cir033
- Lopez A.S., Burnett-Hartman A., Nambiar R. Transmission of a newly characterized strain of varicella-zoster virus from a patient with herpes zoster in a long-term-care facility, West Virginia, 2004. J. Infect. Dis. 2008;197(5):646–53. DOI: https://doi.org/10.1086/527419
- Saidel-Odes L., Borer A., Reisenberg K., et al. An outbreak of varicella in staff nurses exposed to a patient with localized herpes zoster. Scand. J. Infect. Dis. 2010;42(8):620–2. DOI: https://doi.org/10.3109/00365541003754436
- Литяева Л.А., Тен М.Б., Ковалева О.В., Закопаева Е.С. Особенности течения ветряной оспы у детей с иммунодефицитными состояниями. Детские инфекции. 2015;14(4):50–2. Lityaeva L.A., Ten M.B., Kovaleva O.V., Zakopaeva E.S. Peculiarities of varicella in children with immunodeficiency. Children Infections. 2015;14(4):50–2. DOI: https://doi.org/10.22627/2072-8107-2015-14-4-50-52 EDN: https://elibrary.ru/uxqebp
- Daley A.J., Thorpe S., Garland S.M. Varicella and the pregnant woman: prevention and management. Aust. N.Z. J. Obstet. Gynaecol. 2008;48(1):26–33. DOI: https://doi.org/10.1111/j.1479-828X.2007.00797.x
- Sarit S., Shruti S., Deepinder C., Chhina R.S. Chicken pox outbreak in the Intensive Care Unit of a tertiary care hospital: lessons learnt the hard way. Indian J. Crit. Care Med. 2015;19(12):723–5. DOI: https://doi.org/10.4103/0972-5229.171397
- Talebi-Taher M., Noori M., Shamshiri A.R., Barati M. Varicella Zoster antibodies among health care workers in a university hospital, Teheran, Iran. Int. J. Occup. Med. Environ. Health. 2010;23(1):27–32. DOI: https://doi.org/10.2478/v10001-010-0011-x
- Centers for Disease Control and Prevention. Immunization of health care personnel: recommendation of the Advisory Committee on Immunization Practices (AICP). MMWR Recomm. Rep. 2011;60(RR-7):1–45.
- WHO. Varicella and herpes zoster vaccines: WHO position paper; 2014. URL: https://www.who.int/publications/i/item/who-wer-8925-265-288
- Amjadi O., Rafiei A., Haghshenas M., et al. A systematic review and meta-analysis of seroprevalence of varicella zoster virus: A nationwide population-based study. J. Clin. Virol. 2017;87:49–59. DOI: https://doi.org/10.1016/j.jcv.2016.12.001
- Афонина Н.М. Эпидемиологическая характеристика и меры профилактики инфекции, вызванной вирусом Varicella zoster: Автореф. дисс. … канд. мед. наук. М.; 2019. Afonina N.M. Epidemiological characteristics and measures of prevention of infection caused by the Varicella zoster virus: Diss. Moscow; 2019.
- Афонина Н.М., Михеева И.В., Михеева М.А. Ветряная оспа в медицинских организациях Москвы. В кн.: Инфекционные болезни в современном мире: эволюция, текущие и будущие угрозы: сборник трудов XV Ежегодного Всероссийского конгресса по инфекционным болезным имени академика В.И. Покровского. М.; 2023. Afonina N.M., Mikheeva I.V., Mikheeva M.A. Chicken pox in medical organizations in Moscow. In: Infectious Diseases in the Modern World: Evolution, Current and Future Threats: Proceedings of the XV Annual All-Russian Congress on Infectious Diseases named after Academician V.I. Pokrovsky. Moscow; 2023. EDN: https://elibrary.ru/ovafrv
- Национальное научное общество инфекционистов. Клинические рекомендации «Ветряная оспа у взрослых»; 2014.
- Koshy E., Mengting L., Kumar H., Jianbo W. Epidemiology, treatment and prevention of herpes zoster: A comprehensive review. Indian J. Dermatol. Venereol. Leprol. 2018;84(3):251–62. DOI: https://doi.org/10.4103/ijdvl.IJDVL_1021_16
- Ермоленко М.В. Серологический мониторинг в системе эпидемиологического надзора за ветряной оспой: Автореф. дисс. … канд. мед. наук. М.; 2014. Ermolenko M.V. Serological monitoring in the system of epidemiological surveillance of chickenpox: Diss. Moscow; 2014.
- Biskupska M., Małecka I., Stryczyńska-Kazubska J., Wysocki J. Varicella — a potential threat to maternal and fetal health. Ginekol. Pol. 2017;88(1):13–9. DOI: https://doi.org/10.5603/gp.a2017.0003
Supplementary files

